



Cocaine withdrawal begins within one to two hours of the last use and follows a predictable pattern driven by dopamine system collapse. The psychological intensity of the crash surprises most people because cocaine withdrawal produces no dramatic physical symptoms, yet the depression, fatigue, and anhedonia that define acute withdrawal are severe enough to make continued abstinence feel impossible.
Each stage below maps what happens neurologically and clinically from the first-hour crash through the ten-week post-acute withdrawal window. Understanding the timeline makes it possible to plan around each phase rather than be caught off guard by it.
Key Takeaways
- According to SAMHSA’s 2020 National Survey on Drug Use and Health, approximately 1.9 million people aged 12 or older met criteria for cocaine use disorder in the prior year, making it one of the most prevalent stimulant use disorders in the United States.
- The acute cocaine withdrawal crash peaks between Days 1 and 3 after the last use, when dopaminergic dysregulation and D2/D3 receptor downregulation are at their most severe.
- According to the National Institute on Drug Abuse, cocaine blocks the dopamine transporter (DAT), flooding the nucleus accumbens with excess dopamine and establishing the neurological pattern that drives withdrawal upon cessation.
- Post-acute withdrawal syndrome (PAWS) sustains episodic cravings, dysphoria, and low motivation for 3 to 10 weeks after the last use in chronic cocaine users.
- Crack cocaine produces a faster and more intense crash than powder cocaine due to its rapid absorption route and the kindling effect generated by compulsive binge cycling.
What Is Cocaine Withdrawal?
Cocaine withdrawal syndrome is the clinically recognized cluster of psychological and physiological symptoms that emerges when a person with cocaine use disorder abruptly reduces or stops use after prolonged or heavy consumption.
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR) classifies cocaine withdrawal within the stimulant use disorder category and defines it as a condition causing clinically significant distress or functional impairment. Diagnosis requires that symptoms are not attributable to another substance or medical condition.
DSM-5 Criteria for Cocaine Withdrawal Syndrome
The DSM-5 defines cocaine withdrawal as occurring within a few hours to several days following cessation or reduction of heavy cocaine use. The diagnostic criteria require dysphoric mood combined with two or more of the following symptoms:
DSM-5 cocaine withdrawal requires dysphoric mood plus at least two of the following:
- Fatigue and hypersomnia: Cocaine suppresses fatigue through dopamine-driven arousal; cessation removes this stimulation and produces prolonged sleep and persistent low energy.
- Increased appetite: Norepinephrine elevation during cocaine use suppresses hunger; removal of cocaine triggers a pronounced appetite rebound within 24 to 48 hours.
- Psychomotor retardation or agitation: Dopaminergic collapse reduces motor output in most people, producing visible slowing, though some present with restless agitation.
- Vivid and unpleasant dreams: Disruption of dopaminergic REM modulation generates intense, often disturbing dream content during acute and subacute withdrawal.
- Insomnia: Despite hypersomnia during the crash, sleep architecture disruption can produce insomnia in later withdrawal phases.
Why Cocaine Withdrawal Differs from Physical Withdrawal Syndromes
Cocaine withdrawal does not carry the physiological dangers of alcohol or benzodiazepine withdrawal. Seizures, delirium tremens, and life-threatening cardiovascular instability attributable to cocaine cessation alone are not documented in the clinical literature.
What cocaine withdrawal does produce is a severe psychological state driven by dopaminergic collapse. This absence of dramatic physical symptoms creates a clinically dangerous misconception that cocaine withdrawal is minor or self-manageable. The anhedonia and suicidal ideation that can emerge during peak withdrawal make structured clinical support critical.
How Cocaine Disrupts the Dopamine System
Cocaine produces euphoria by binding to the dopamine transporter and blocking dopamine reuptake at the synapse, flooding the nucleus accumbens with excess dopamine and generating an intense reward signal. This mechanism reinforces subsequent cocaine use and drives the compulsive use pattern central to cocaine use disorder.
Chronic cocaine use forces the brain to compensate for sustained dopamine excess by downregulating dopamine D2 and D3 receptors. When cocaine use stops, the brain cannot rapidly restore normal dopamine signaling. The resulting D2/D3 receptor hypofunction creates the reward deficiency state that defines acute cocaine withdrawal.
The Mesolimbic Reward Pathway and Dopaminergic Dysregulation
Cocaine’s disruption of dopamine extends across two major pathways simultaneously. The mesolimbic reward pathway, projecting from the ventral tegmental area to the nucleus accumbens, governs motivational drive and becomes functionally impaired during withdrawal. The mesocortical dopamine pathway, connecting the ventral tegmental area to the prefrontal cortex, regulates executive function and impulse control.
During cocaine withdrawal, mesolimbic pathway depletion generates anhedonia while mesocortical pathway deficiency impairs the prefrontal cognition needed to resist cravings. This dual-pathway dysfunction explains why stimulant use disorder produces both profound emotional pain and the cognitive vulnerability that drives relapse at the same time.

Cocaine Withdrawal Timeline: Hours 1 Through Week 10
The cocaine withdrawal timeline unfolds across five stages, each reflecting the brain’s adaptation to dopamine deficiency. The pace and severity of each stage vary based on frequency of use, duration of use, route of administration, and the presence of co-occurring mental health conditions.
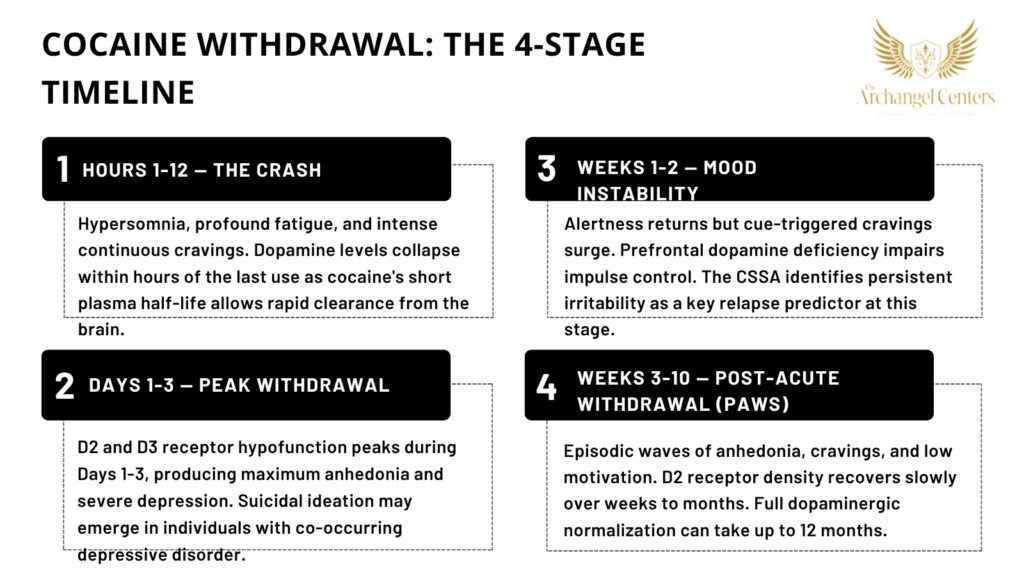
- Stage 1: Hours 1-12 (The Crash Begins) Fatigue, dysphoria, and hypersomnia emerge within one to two hours of the last use as cocaine’s plasma levels fall and dopamine activity collapses. Cocaine’s plasma half-life is approximately one hour, meaning acute dopamine depletion begins almost immediately after the last dose. Irritability, hunger, and a powerful urge to use again to reverse the crash characterize this phase.
- Stage 2: Hours 12-72 / Days 1-3 (Peak Withdrawal) Anhedonia reaches maximum intensity, with D2/D3 receptor hypofunction at its deepest. The person typically experiences severe depression, psychomotor retardation, and an inability to feel pleasure from any source. Suicidal ideation can emerge in individuals with a history of co-occurring depressive disorder during this window, making clinical monitoring critical.
- Stage 3: Days 4-7 (Early Subacute Phase) Acute symptoms begin to lift, but cue-triggered cravings surge as alertness returns and the person re-engages with their environment. Prefrontal dopamine depletion continues to impair impulse control during this phase. Anxiety, agitation, and difficulty concentrating are common as the reward system begins its slow neurological recovery.
- Stage 4: Weeks 1-2 (Mood Instability Phase) Sleep architecture begins to normalize, though vivid dreams and episodic insomnia may persist. The Cocaine Selective Severity Assessment (CSSA), the validated clinical rating scale for cocaine withdrawal severity, identifies persistent irritability and depression at this stage as the strongest predictors of relapse in the following two weeks. Cravings shift from constant to episodic, triggered primarily by environmental cues and emotional stress.
- Stage 5: Weeks 3-10 (Post-Acute Withdrawal Syndrome) Post-acute withdrawal syndrome (PAWS) produces intermittent waves of depression, low motivation, and intense cravings as D2 receptor density recovers slowly toward baseline. Dopamine receptor recovery in the striatum can require 12 months or longer in heavy users, according to neuroimaging research. Functional improvement in mood and cognition typically precedes full receptor normalization by several months.
Cocaine Withdrawal Symptoms by Severity
Cocaine withdrawal symptoms follow the timeline above and vary in presentation based on duration of use, frequency, the presence of co-occurring mental health conditions, and whether crack cocaine or powder cocaine was used. The three tiers below reflect the clinical range from expected withdrawal to presentations requiring immediate support.
Common Cocaine Withdrawal Symptoms
During the first two weeks of cocaine withdrawal, the following symptoms occur in most people:
Common cocaine withdrawal symptoms include:
- Fatigue and hypersomnia: Dopamine-driven arousal collapses after cocaine cessation, producing extended sleep and persistent low energy that can be mistaken for clinical depression.
- Dysphoria and depressed mood: D2/D3 receptor downregulation removes the brain’s capacity to generate positive affect, creating a pervasive flatness neurologically distinct from situational sadness.
- Intense, episodic cravings: Conditioned dopamine responses in the nucleus accumbens produce powerful urges triggered by environmental cues, people, or emotional states associated with prior use.
- Increased appetite and weight gain: Norepinephrine-mediated appetite suppression reverses upon cocaine cessation, producing a pronounced hunger rebound within the first 24 to 48 hours.
- Cognitive slowing: Mesocortical dopamine depletion impairs working memory, attention, and decision-making during the first one to two weeks of withdrawal.
Severe Cocaine Withdrawal Symptoms
The following symptoms indicate psychological distress requiring immediate clinical contact:
Severe cocaine withdrawal symptoms requiring same-day clinical evaluation:
- Suicidal ideation or self-harm urges: Cocaine withdrawal can precipitate a major depressive episode in vulnerable individuals. Anyone experiencing suicidal thoughts during cocaine withdrawal should contact the 988 Suicide and Crisis Lifeline immediately by call or text. This lifeline is available 24 hours a day.
- Psychosis persisting beyond 48 hours: High-dose cocaine use can produce paranoid delusions and hallucinations. Psychosis that does not resolve within 48 hours of cessation may indicate an underlying condition requiring specialized clinical evaluation.
- Severe agitation and behavioral dysregulation: Norepinephrine rebound during the crash can produce hostility and impulsive behavior that places the person or those around them at risk.
- Chest pain or cardiac symptoms: Cocaine’s cardiovascular effects can trigger panic attacks during withdrawal that include palpitations and chest pain, requiring medical evaluation to rule out myocardial involvement.
Long-Term Effects and Post-Acute Withdrawal Syndrome
Post-acute withdrawal syndrome from cocaine use disorder typically spans Weeks 3 through 10, with heavy long-term users experiencing episodic symptoms beyond this window. PAWS does not present as continuous distress; it arrives in waves of varying intensity that diminish over time.
Long-term effects associated with cocaine PAWS include:
- Protracted anhedonia: D2 receptor density recovers slowly, sustaining the reward deficiency state for weeks to months. Activities that previously produced pleasure, including exercise and social engagement, may feel unrewarding during this recovery period.
- Cue-triggered craving episodes: Environmental stimuli linked to prior cocaine use activate conditioned dopamine responses in the nucleus accumbens, producing sudden and intense urges that are not reliably controlled through willpower alone.
- Mood cycling and depressive episodes: PAWS-related mood instability can resemble bipolar II disorder or cyclothymia. Accurate clinical evaluation during this window prevents misdiagnosis and incorrect pharmacological treatment.
- Protracted cognitive recovery: Prefrontal cortex function, including impulse control and working memory, continues to improve for 12 to 24 weeks after the last cocaine use, provided abstinence is maintained.
Crack Cocaine vs. Powder Cocaine: Does the Timeline Differ?
The core stages of cocaine withdrawal are present in both cocaine hydrochloride (powder cocaine) and crack cocaine (freebase cocaine) users, but the intensity, pace, and crash severity differ meaningfully between the two forms.
| Factor | Powder Cocaine | Crack Cocaine |
|---|---|---|
| Route of administration | Intranasal | Smoked |
| Onset of high | 3 to 5 minutes | 8 to 10 seconds |
| Duration of high | 15 to 30 minutes | 5 to 10 minutes |
| Crash onset after last use | 30 to 60 minutes | 10 to 20 minutes |
| Typical use pattern | Episodic | Compulsive binge cycling |
| Kindling effect | Moderate | Pronounced |
| Withdrawal intensity | Moderate to severe | Severe to very severe |
Crack cocaine’s shorter duration of action drives compulsive binge cycling, in which repeated dosing within a short window attempts to prevent or reverse the crash. Each successive binge further depletes dopamine stores in the nucleus accumbens and intensifies the kindling effect. This escalating pattern elevates the risk of co-occurring stimulant-induced mood disorder and increases the severity and duration of PAWS following cessation.
Cocaine Use Disorder Treatment at Archangel Centers
Archangel Centers provides structured outpatient treatment for cocaine use disorder at its Tinton Falls, New Jersey location, with levels of care spanning from the acute crash phase through the post-acute withdrawal window.
Partial Care Program
Archangel’s Partial Care program runs Monday through Saturday and provides the highest level of outpatient structure for the early weeks of cocaine withdrawal. Programming targets anhedonia, mood instability, and cognitive impairment through DBT skills training, relapse prevention groups, and cognitive behavioral therapy that directly addresses the cue-triggered craving patterns established by cocaine use disorder.
Intensive Outpatient Program
Archangel’s Intensive Outpatient Program is designed for clients entering the subacute and PAWS stages of cocaine withdrawal, providing three to five days per week of structured clinical programming. Group and individual sessions target the cue-triggered cravings, mood cycling, and executive function deficits that drive relapse during Weeks 2 through 10 of the withdrawal timeline.
Virtual IOP
Archangel’s Virtual IOP delivers the same evidence-based clinical programming through a telehealth platform, extending structured cocaine withdrawal support to clients throughout New Jersey. This level of care is well-suited to the PAWS phase, when cravings are episodic and clients are rebuilding work and family routines.
Dual Diagnosis Treatment
Co-occurring major depressive disorder, generalized anxiety disorder, and stimulant-induced mood disorder frequently accompany cocaine use disorder and become more apparent during the PAWS phase. Archangel’s dual diagnosis program integrates psychiatric evaluation and medication management with cocaine-specific clinical programming, ensuring that PAWS-related mood symptoms are correctly attributed rather than misdiagnosed as a primary mood disorder. Same-day assessments are available for individuals ready to begin.
Frequently Asked Questions
When Is the Peak of Cocaine Withdrawal?
Cocaine withdrawal peaks between Days 1 and 3 after the last use. During this window, dopamine D2/D3 receptor hypofunction is at its most severe, producing maximum anhedonia, depression, and fatigue. Most people report that acute symptoms begin to lift noticeably by Days 4 through 5, though mood instability continues for one to two weeks following the peak.
What Happens to Your Body After Quitting Cocaine?
After quitting cocaine, the brain’s dopamine transporter begins normalizing within one to two weeks. D2 and D3 receptor density recovers more slowly, over several weeks to months. Physical effects include rebound hunger, disrupted sleep, and fatigue as the body recalibrates after cocaine’s suppression of normal physiological processes. Cognitive function and impulse control continue improving for up to six months.
How Long Does It Take for Dopamine to Reset After Cocaine?
Dopamine transporter levels begin normalizing within one to two weeks of abstinence. D2/D3 receptor downregulation, the primary driver of anhedonia, recovers over four to twelve weeks in most people. Prefrontal dopamine function governing impulse control and decision-making continues to improve for up to six months. Heavy long-term use extends all of these timelines significantly.
Is There a Withdrawal Scale for Cocaine?
The Cocaine Selective Severity Assessment (CSSA) is the validated clinical instrument for measuring cocaine withdrawal severity. It evaluates 18 symptoms including dysphoria, sleep disturbance, cravings, and cognitive impairment. Clinicians use CSSA scores to guide treatment intensity decisions and monitor recovery trajectory. It is the standard measurement instrument used in cocaine withdrawal clinical research.
Can Cocaine Withdrawal Cause Suicidal Thoughts?
Cocaine withdrawal can precipitate suicidal ideation, particularly in people with a history of depression or co-occurring mental health conditions. The D2 receptor downregulation that drives anhedonia during withdrawal can produce a depressive state clinically indistinguishable from major depressive disorder. Anyone experiencing suicidal thoughts during cocaine withdrawal should contact the 988 Suicide and Crisis Lifeline immediately by call or text.
How Long Does Cocaine PAWS Last?
Post-acute withdrawal syndrome from cocaine use disorder typically spans three to ten weeks after the last use. Heavy long-term users, particularly those with a history of crack cocaine binge cycling, may experience episodic symptoms for three to six months. PAWS does not present as continuous distress; it arrives in waves of craving, dysphoria, and low motivation that diminish in frequency and intensity over time.
References
- National Institute on Drug Abuse. (2021). Cocaine DrugFacts. U.S. Department of Health and Human Services. https://nida.nih.gov/publications/drugfacts/cocaine
- Substance Abuse and Mental Health Services Administration. (2021). Key Substance Use and Mental Health Indicators in the United States: Results from the 2020 National Survey on Drug Use and Health (HHS Publication No. PEP21-07-01-003). Center for Behavioral Health Statistics and Quality. https://www.samhsa.gov/data/sites/default/files/reports/rpt35325/NSDUHFFRPDFWHTMLFiles2020/2020NSDUHFFR1PDFW102121.pdf
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). American Psychiatric Association Publishing.
- Kampman, K. M., Volpicelli, J. R., McGinnis, D. E., Alterman, A. I., Weinrieb, R. M., D’Angelo, L., & Epperson, L. E. (1998). Reliability and validity of the Cocaine Selective Severity Assessment. Addictive Behaviors, 23(4), 449-461.
- Koob, G. F., & Volkow, N. D. (2016). Neurobiology of addiction: A neurocircuitry analysis. The Lancet Psychiatry, 3(8), 760-773.
- Substance Abuse and Mental Health Services Administration. (2015). Detoxification and Substance Abuse Treatment. Treatment Improvement Protocol (TIP) Series, No. 45. Center for Substance Abuse Treatment. https://store.samhsa.gov/product/tip-45-detoxification-and-substance-abuse-treatment/sma15-4131
- Volkow, N. D., Wang, G. J., Fowler, J. S., & Tomasi, D. (2012). Addiction circuitry in the human brain. Annual Review of Pharmacology and Toxicology, 52, 321-336.