



Meth withdrawal starts later than most people expect and lasts far longer than the crash itself suggests. The acute crash emerges within 24 to 48 hours of the last use, driven by the collapse of dopamine stores that methamphetamine depleted over months or years of compulsive use. What follows extends well beyond the first week.
The timeline below maps each stage of methamphetamine withdrawal from the initial crash through the post-acute withdrawal window and explains why sleep, motivation, and cognition are the slowest functions to recover.
Key Takeaways
- According to the National Institute on Drug Abuse, heavy meth use damages the brain’s dopamine system, cutting key receptors in half. Healing takes months or even years of staying off the drug, which is why people often feel flat, joyless, and mentally foggy long after the initial crash is over.
- The meth crash peaks between Days 1 and 3 and is defined by hypersomnia, severe dysphoria, and profound fatigue as striatal dopamine levels collapse below functional thresholds.
- Post-acute withdrawal syndrome (PAWS) from methamphetamine use disorder produces episodic depression, cravings, and executive function deficits for one to three months in moderate users and up to 12 months in heavy, long-term users.
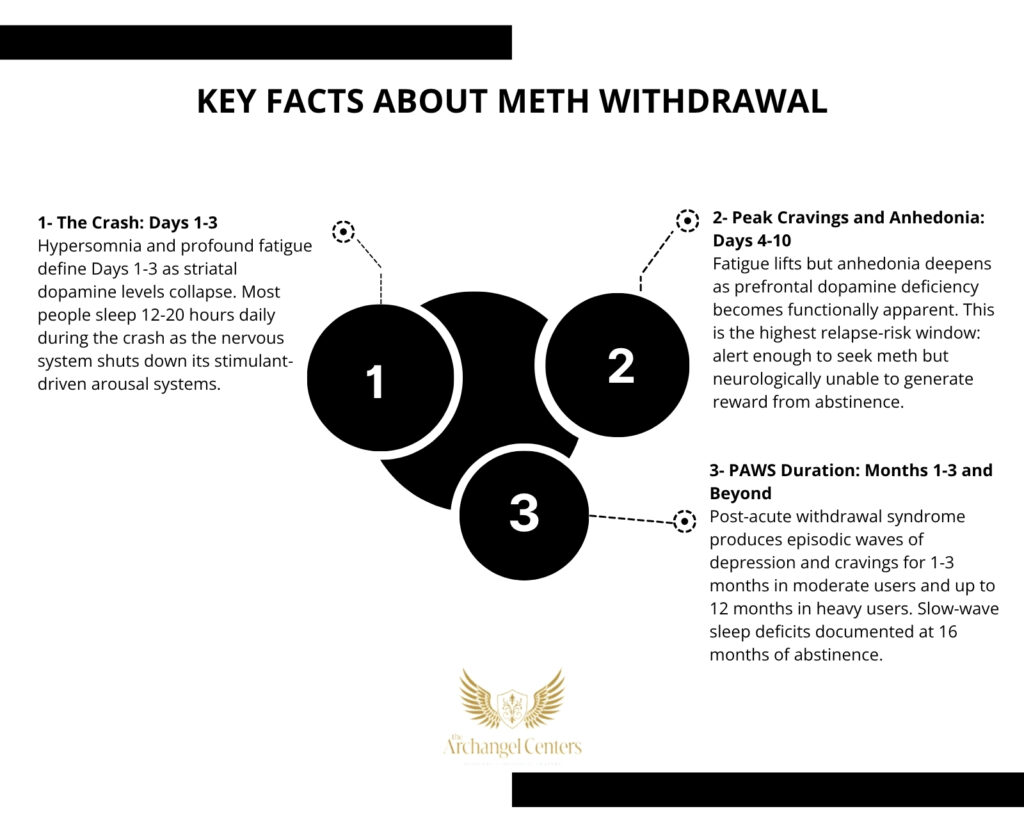
- Slow-wave sleep deficits from methamphetamine use are documented in neuroimaging studies at 16 months of abstinence, making sleep the slowest-recovering symptom category in the entire withdrawal timeline.
Why Meth Withdrawal Differs from Other Stimulant Withdrawal
Methamphetamine withdrawal produces a more severe and prolonged neurological disruption than cocaine withdrawal, despite both substances falling under stimulant use disorder in the DSM-5-TR. The difference lies in the mechanism of damage.
How Methamphetamine Depletes Dopamine Stores
Cocaine produces excess dopamine by blocking the dopamine transporter (DAT) without depleting stored reserves. Methamphetamine operates through a fundamentally more destructive mechanism: it forces dopamine out of vesicular storage and floods the synapse while simultaneously blocking reuptake, rapidly exhausting the brain’s entire available dopamine supply.
Chronic methamphetamine use causes structural damage to dopaminergic axon terminals in the striatum and prefrontal cortex. Neuroimaging studies document DAT reductions of up to 50% in heavy users evaluated for stimulant use disorder. This structural damage extends the withdrawal recovery timeline well beyond what receptor adaptation alone would produce, and it explains why meth withdrawal is longer and harder than cocaine withdrawal despite both being stimulants.
Why the Meth Crash Arrives Later
Methamphetamine’s plasma half-life is approximately 10 to 12 hours, compared to cocaine’s half-life of approximately one hour. The meth crash therefore arrives 24 to 48 hours after the last dose rather than within 90 minutes. This delay produces a clinically dangerous misconception: many people feel relatively functional for the first several hours after stopping and interpret this as mild withdrawal. The calm before the dopaminergic collapse resolves is not a sign of easy withdrawal. It is pharmacokinetics.
Meth Withdrawal Timeline: Days 1 Through Month 3
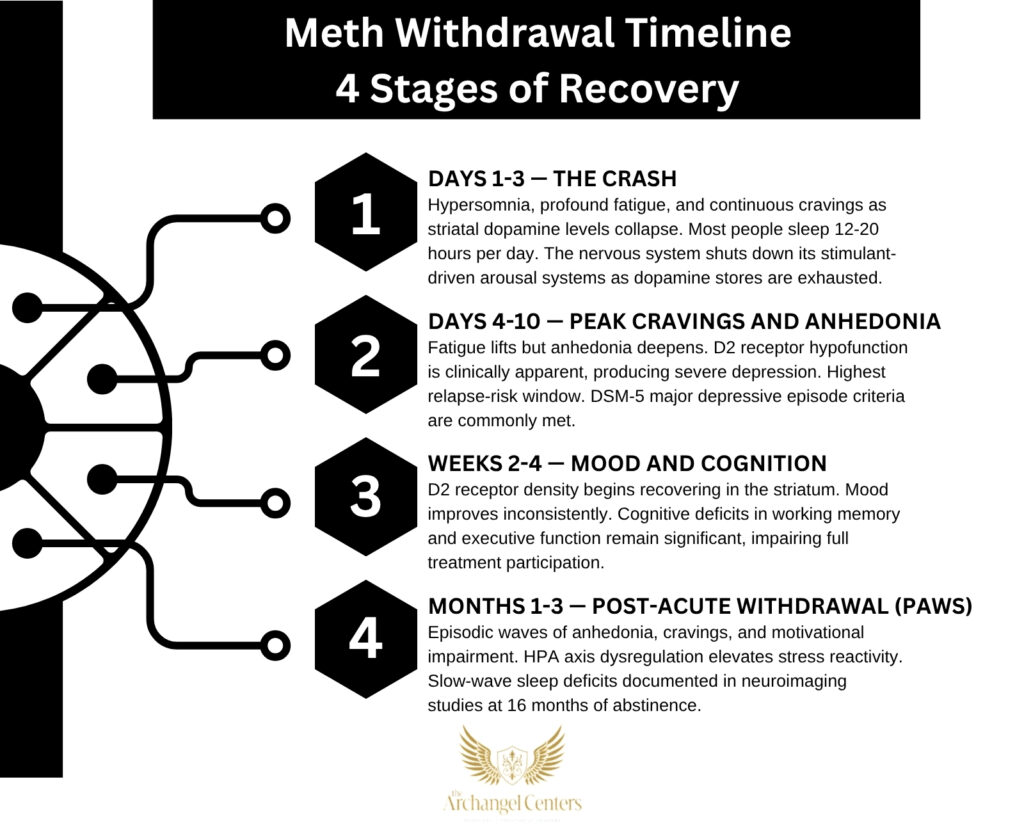
The methamphetamine withdrawal timeline unfolds across four stages. Severity depends on duration of use, daily dose, route of administration, and the presence of co-occurring mental health conditions.
- Stage 1: Days 1-3 (The Crash) Hypersomnia, profound fatigue, and intense dysphoria define the first 72 hours as striatal dopamine levels collapse and the brain’s arousal systems shut down. Most people sleep for 12 to 20 hours per day during this stage. Cravings are continuous and urgent. Mood is severely dysphoric, characterized by emotional emptiness rather than classical sadness. The dopaminergic void of the crash phase is the neurological foundation upon which the subsequent stages build.
- Stage 2: Days 4-10 (Peak Cravings and Anhedonia) Fatigue lifts but anhedonia deepens as the prefrontal cortex’s dopamine deficit becomes functionally apparent with the return of wakefulness. This is the highest-risk stage for relapse because the person is now alert enough to seek out meth but neurologically incapable of generating motivation, reward, or satisfaction from anything else. DSM-5-defined major depressive episodes are common at this stage. Cue-triggered cravings surge with re-exposure to the environment associated with prior use.
- Stage 3: Weeks 2-4 (Mood and Cognition) Dopamine D2 receptor density begins recovering in the striatum, producing a gradual and inconsistent improvement in mood. Cognitive deficits in working memory, processing speed, and executive function remain clinically significant and impair full participation in treatment programming. Sleep remains fragmented with slow-wave sleep deficits and REM rebound producing vivid, often disturbing dreams. Cravings shift from constant to episodic and cue-triggered.
- Stage 4: Months 1-3 (PAWS) Post-acute withdrawal syndrome from methamphetamine use disorder produces waves of anhedonia, intense cravings, and motivational impairment for one to three months in moderate users, and up to 12 months in heavy users. The defining PAWS pattern is prolonged emotional flatness at baseline interrupted by episodic craving surges triggered by stress, environmental cues, or sleep disruption. Each wave diminishes in intensity as dopaminergic recovery progresses.
Meth Withdrawal Symptoms by Severity
Methamphetamine withdrawal symptoms vary in clinical presentation based on duration of use, daily dose, and the presence of co-occurring conditions. The three tiers below reflect the range from expected withdrawal to presentations requiring immediate clinical intervention.
Common Meth Withdrawal Symptoms
During the first two to four weeks of methamphetamine withdrawal, the following symptoms occur in most people:
Common meth withdrawal symptoms include:
- Hypersomnia and profound fatigue: Methamphetamine suppresses adenosine-mediated sleep pressure; cessation removes this suppression and produces extended sleep periods and persistent daytime fatigue lasting several weeks.
- Anhedonia and emotional flatness: Striatal dopamine depletion removes the brain’s capacity to register reward, making food, social connection, exercise, and other normally reinforcing activities feel meaningless or unrewarding.
- Increased appetite and weight gain: Norepinephrine elevation during meth use suppresses hunger; removal of methamphetamine triggers a pronounced appetite rebound with significant caloric overeating common in the first one to two weeks.
- Cognitive impairment: Prefrontal dopamine deficiency impairs working memory, attention, and decision-making during the subacute phase, impairing treatment participation and increasing vulnerability to cue-triggered relapse.
- Episodic cravings: Conditioned dopamine responses in the nucleus accumbens produce intense, sudden urges triggered by environmental stimuli linked to prior methamphetamine use.
Severe Meth Withdrawal Symptoms
The following presentations require immediate clinical evaluation:
Severe meth withdrawal symptoms requiring same-day contact with a treatment provider:
- Suicidal ideation: The anhedonia and hopelessness of the crash and PAWS phases can precipitate suicidal ideation, particularly in individuals with pre-existing depressive vulnerability. Anyone experiencing thoughts of suicide during meth withdrawal should contact the 988 Suicide and Crisis Lifeline immediately by call or text.
- Stimulant-induced psychosis beyond 72 hours: Methamphetamine use can trigger paranoid delusions, auditory hallucinations, and thought disorganization. Psychosis resolving within 72 hours of the last use is consistent with stimulant-induced psychosis. Psychosis persisting beyond 72 hours requires psychiatric evaluation to rule out a primary condition such as schizoaffective disorder.
- Severe agitation and hostility: Noradrenergic dysregulation during early withdrawal produces behavioral dyscontrol in some individuals that creates safety risks requiring a structured clinical setting to manage.
- Cardiovascular symptoms: Meth-related arrhythmias and hypertensive episodes can persist into early withdrawal and require medical evaluation separate from addiction treatment.
Long-Term Effects and Meth PAWS
Methamphetamine post-acute withdrawal syndrome produces functional impairment that extends well beyond acute withdrawal in heavy users:
Long-term effects during the meth recovery period include:
- Protracted anhedonia: DAT and D2 receptor recovery in the striatum progresses over months. Neuroimaging studies document measurable functional improvement at 12 to 24 months of abstinence, but subjective anhedonia frequently outlasts structural recovery due to the gap between receptor normalization and behavioral recalibration.
- Executive function deficits: Prefrontal cortex recovery is among the slowest processes in meth withdrawal. Working memory, impulse control, and decision-making remain below premorbid baseline for six to 12 months of sustained abstinence in heavy users.
- Mood cycling and depressive episodes: PAWS-related mood instability produces intermittent depressive and euthymic states. Accurate clinical assessment distinguishes PAWS-driven mood symptoms from a primary co-occurring mood disorder requiring dual diagnosis care.
- Elevated stress reactivity: Chronic methamphetamine use dysregulates the hypothalamic-pituitary-adrenal (HPA) axis, sensitizing the stress response and making PAWS-phase individuals significantly more reactive to environmental stressors than the general population.
Why Sleep Takes the Longest to Return After Meth
Sleep disruption is among the most clinically underaddressed consequences of methamphetamine withdrawal and the symptom category with the slowest documented recovery trajectory.
Methamphetamine directly suppresses slow-wave sleep (SWS), the deepest non-REM stage governing cellular repair, immune function, and declarative memory consolidation. Chronic meth use progressively eliminates SWS, forcing the brain to sustain arousal through stimulant-driven dopamine and norepinephrine activation rather than normal restorative sleep cycling.
Upon cessation, the brain attempts to simultaneously rebalance adenosine-mediated sleep pressure, REM homeostasis, and SWS architecture. REM rebound produces vivid, disturbing dreams that disrupt sleep quality even when total sleep duration increases during the crash. Neuroimaging research has documented measurable SWS deficits in methamphetamine-abstinent individuals at 16 months of sobriety, confirming that sleep architecture recovery follows a slower trajectory than dopamine receptor normalization alone.
Sleep deprivation during the recovery period amplifies cue-triggered cravings, impairs the cognitive recovery needed to benefit fully from behavioral therapy, and substantially elevates relapse risk. Addressing sleep as a clinical priority from Week 1 of treatment is not ancillary care; it is a direct relapse prevention intervention.
Why Detox Alone Is Not Enough for Meth Recovery
Medically supervised detox addresses the acute crash phase of methamphetamine withdrawal but does not intervene at the stages where relapse risk is highest.
The peak cue-triggered craving window in Stages 2 and 3 of the timeline coincides with the prefrontal dopamine deficit that most severely impairs impulse control. A person who leaves structured care after detox re-enters the same environment, social networks, and emotional patterns that conditioned their use at the precise neurological moment when their capacity to resist those cues is lowest.
Cognitive behavioral therapy (CBT) and contingency management are the most evidence-supported psychosocial interventions for methamphetamine use disorder and produce outcomes significantly superior to detox alone. Both modalities produce the greatest benefit when delivered consistently across the 8 to 12 weeks spanning Stages 2 through 4 of the withdrawal timeline, which is precisely the window that outpatient programming is designed to cover.
Methamphetamine Use Disorder Treatment at Archangel Centers
Archangel Centers provides structured outpatient treatment for methamphetamine use disorder at its Tinton Falls, New Jersey location, with three levels of care aligned with the meth withdrawal timeline from the crash phase through PAWS.
Partial Care Program
Archangel’s Partial Care program runs Monday through Saturday and delivers the most intensive level of outpatient structure during the critical first two to four weeks of meth withdrawal. Daily programming targets anhedonia, cue-triggered cravings, and cognitive impairment through CBT groups, DBT skills training, and relapse prevention curricula designed specifically for the dopaminergic recovery phase of stimulant withdrawal.
Intensive Outpatient Program
Archangel’s Intensive Outpatient Program provides three to five days per week of structured clinical support across the subacute and PAWS phases of methamphetamine withdrawal. Programming targets the mood cycling, executive function deficits, and cue-triggered cravings that drive relapse during Weeks 2 through 12, while clients maintain work, family, and daily responsibilities.
Virtual IOP
Archangel’s Virtual IOP delivers the same evidence-based programming through a telehealth platform for clients throughout New Jersey who cannot attend daily in-person treatment. This level of care is well-suited to the PAWS phase, when structured clinical support remains essential but intensive daily attendance is not required. Same-day assessments are available for anyone ready to begin.
Frequently Asked Questions
How Long Do Meth Withdrawal Symptoms Last?
Acute meth withdrawal symptoms resolve within one to two weeks for most people. Post-acute withdrawal syndrome extends the timeline, producing episodic depression, cravings, and cognitive impairment for one to three months in moderate users. Heavy, long-term methamphetamine users report PAWS symptoms at six to twelve months. Sleep architecture disruption is the slowest-resolving symptom and can persist beyond 16 months.
What Are the Stages of Stimulant Withdrawal?
Methamphetamine withdrawal progresses through four stages: the crash (Days 1 to 3), peak cravings and anhedonia (Days 4 to 10), subacute mood and cognitive recovery (Weeks 2 to 4), and post-acute withdrawal syndrome (Months 1 to 3 and beyond). Each stage reflects a distinct phase of dopaminergic and noradrenergic recovery and calls for different clinical interventions to manage effectively.
Can Meth Withdrawal Cause Psychosis?
Stimulant-induced psychosis from methamphetamine is well-documented and typically includes paranoid delusions, auditory hallucinations, and disorganized thinking. Psychosis resolving within 72 hours of the last dose is classified as stimulant-induced and does not indicate a primary psychotic disorder. Psychosis persisting beyond 72 hours requires psychiatric evaluation to determine whether a co-occurring condition such as schizoaffective disorder is present.
What Helps With Meth Withdrawal Symptoms?
No FDA-approved pharmacotherapy exists specifically for methamphetamine withdrawal. Cognitive behavioral therapy and contingency management are the most evidence-supported interventions, directly targeting cue-triggered cravings and reinforcing abstinence. Sleep hygiene support, regular aerobic exercise, and nutritional rehabilitation address the physical symptoms of withdrawal and accelerate functional recovery during the subacute phase.
How Long Does Meth PAWS Last?
Post-acute withdrawal syndrome from methamphetamine use disorder spans one to three months in moderate users. Heavy, long-term users experience episodic symptoms for six to twelve months. Meth PAWS does not present as continuous distress. It arrives in waves of anhedonia and cravings that diminish in frequency and intensity as dopamine transporter and D2 receptor density recovers in the striatum.
References
- National Institute on Drug Abuse. (2019). Methamphetamine DrugFacts. U.S. Department of Health and Human Services. https://nida.nih.gov/publications/drugfacts/methamphetamine
- Substance Abuse and Mental Health Services Administration. (2021). Key Substance Use and Mental Health Indicators in the United States: Results from the 2020 National Survey on Drug Use and Health (HHS Publication No. PEP21-07-01-003). https://www.samhsa.gov/data/sites/default/files/reports/rpt35325/NSDUHFFRPDFWHTMLFiles2020/2020NSDUHFFR1PDFW102121.pdf
- McGregor, C., Srisurapanont, M., Jittiwutikarn, J., Laobhripatr, S., Wongtan, T., & White, J. M. (2005). The nature, time course and severity of methamphetamine withdrawal. Addiction, 100(9), 1320-1329.
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). American Psychiatric Association Publishing.
- Volkow, N. D., Chang, L., Wang, G. J., Fowler, J. S., Leonido-Yee, M., Franceschi, D., & Miller, E. N. (2001). Association of dopamine transporter reduction with psychomotor impairment in methamphetamine abusers. American Journal of Psychiatry, 158(3), 377-382.
- Drug Enforcement Administration. (2020). Methamphetamine. U.S. Department of Justice. https://www.dea.gov/factsheets/methamphetamine
- Rawson, R. A., Gonzales, R., & Brethen, P. (2002). Treatment of methamphetamine use disorders: An update. Journal of Substance Abuse Treatment, 23(2), 145-150.