




An addiction treatment center provides structured clinical care that helps adults with substance use disorder stop using substances, address underlying mental health conditions, and build the skills needed for lasting recovery.
Most people delay getting help because they don’t know what to expect. The fear of the unknown is one of the most documented barriers to treatment entry. Understanding what actually happens inside a treatment center removes that barrier.
Treatment at a center like Archangel Centers in New Jersey is not punitive, clinical in the cold sense, or one-size-fits-all. It is structured, individualized, and designed around the specific clinical needs each person brings through the door.
Key Takeaways
- According to SAMHSA, fewer than 10% of adults in the United States who need treatment for substance use disorder receive it in a given year, with fear and stigma consistently cited as primary barriers to entry.
- The National Institute on Drug Abuse reports that addiction treatment produces outcomes comparable to treatment for other chronic conditions such as hypertension, diabetes, and asthma when evidence-based protocols are followed.
- Addiction treatment centers provide care across a clinical continuum ranging from Partial Hospitalization at ASAM Level 2.5 to Intensive Outpatient and standard outpatient programs at lower intensity levels.
- A biopsychosocial assessment conducted at intake determines the ASAM Level of Care appropriate for each client, rather than a self-selected program level.
- Co-occurring disorders involving both substance use disorder and a psychiatric diagnosis such as major depressive disorder or PTSD are present in more than half of adults entering treatment, making integrated dual diagnosis care a clinical standard.
What Is an Addiction Treatment Center?
An addiction treatment center is a specialized clinical facility providing structured therapeutic and medical care to individuals with substance use disorder and co-occurring psychiatric conditions.
What Treatment Centers Do and Do Not Provide
Addiction treatment centers are not hospitals, jails, or institutions for involuntary confinement. Adults enter treatment voluntarily and participate in individualized clinical programming designed to address both the substance use disorder and whatever underlying conditions are driving it.
At Archangel Centers, the conditions treated include alcohol use disorder, opioid use disorder, stimulant use disorder, benzodiazepine dependence, and co-occurring disorders involving psychiatric diagnoses such as major depressive disorder, generalized anxiety disorder, PTSD, and bipolar disorder.
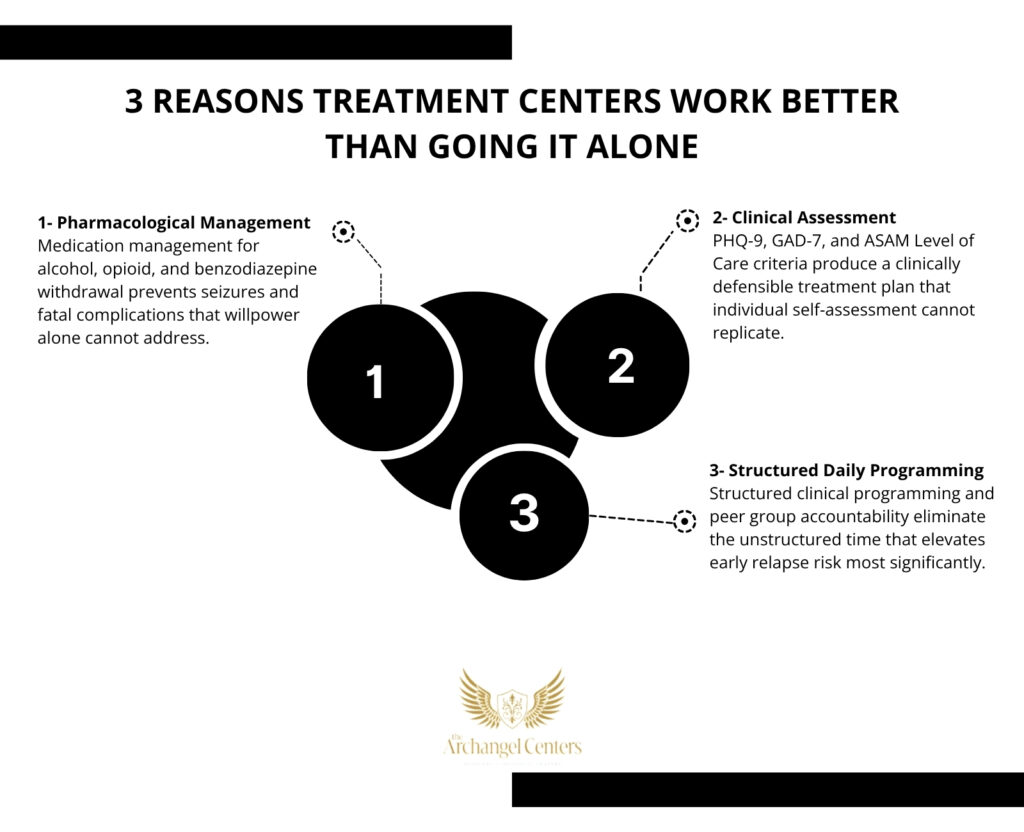
Why Treatment Centers Produce Better Outcomes Than Going It Alone
Substance use disorder is classified as a chronic relapsing brain condition by the American Society of Addiction Medicine. Neuroadaptation from repeated substance exposure alters dopaminergic reward circuitry, prefrontal cortical function, and stress response systems in ways that make self-directed recovery extremely difficult without clinical support.
Treatment centers provide the pharmacological management, behavioral therapy, psychiatric stabilization, and structured peer accountability that individual willpower alone cannot replicate.
Step 1: The First Call and Clinical Assessment
Every treatment experience begins with a single call or online inquiry — a judgment-free, confidential initial contact with an admissions team trained to answer questions about the process, not to pressure a decision.
What the Intake Assessment Covers
The clinical assessment, also called a biopsychosocial assessment, is the foundational document that drives every clinical decision that follows. It is completed during the first clinical contact and reviewed collaboratively with the client before any program begins.
A comprehensive intake assessment covers the following domains:
- Substance use history: substances used, frequency, quantity, duration, and most recent use date.
- Mental health history: prior diagnoses, current psychiatric symptoms, medication history, and any documented trauma history.
- Medical history: physical health conditions, current medications, and any immediate medical needs requiring attention before treatment begins.
- Treatment history: prior treatment episodes, what worked, what did not, and the circumstances surrounding any relapses.
- Social and environmental context: housing stability, employment, family support, legal involvement, and financial considerations.
Standardized screening tools including the PHQ-9 for depression and GAD-7 for anxiety quantify psychiatric symptom severity and help calibrate the level of psychiatric monitoring the client requires during treatment.
ASAM Level of Care Determination
The biopsychosocial assessment maps directly onto ASAM Level of Care criteria, producing a clinically defensible recommendation for whether the client needs detox, residential care, Partial Hospitalization, Intensive Outpatient, or standard outpatient programming.
This determination, not a client’s initial preference or insurance tier, is the primary driver of which program is the right clinical match.
Step 2: Detox and Stabilization
Medical detox is the first clinical step for any client physically dependent on alcohol, benzodiazepines, or opioids, where cessation without pharmacological management carries documented seizure risk or other serious complications.
What Detox Involves and When It Is Required
Alcohol withdrawal syndrome activates GABA-A receptor rebound hyperexcitability, producing seizure risk that peaks between 24 and 72 hours after the last drink. Benzodiazepine withdrawal follows a similar mechanism with extended risk windows. Opioid withdrawal, while rarely fatal, produces severe physiological distress that drives relapse without pharmacological support.
Archangel Centers coordinates medical detox placement with trusted clinical partners for clients who require it. Clients transfer directly into Archangel Centers’ structured programming after medical stabilization, eliminating the treatment gap that most commonly drives relapse.
Stimulant use disorder and cannabis use disorder do not produce physiological withdrawal requiring medical management, though post-acute withdrawal syndrome involving mood disturbance and cognitive disruption may persist for weeks to months after cessation.
Step 3: Entering the Right Level of Care
Following detox or at initial assessment for clients who do not require detox, clients enter a structured clinical program matched to their ASAM Level of Care determination.
Partial Care Program
The Partial Care program is the highest outpatient level, providing 20 to 30 hours of structured clinical treatment per week without requiring overnight stay. It is appropriate for adults who are medically stable, require intensive daily programming, and have access to a structured living environment.
Partial Care at Archangel Centers includes individual therapy, CBT and DBT group therapy, dual diagnosis programming, psychiatric medication management, relapse prevention, and mindfulness-based awareness skill development delivered Monday through Saturday.
Intensive Outpatient Program
The Intensive Outpatient Program provides 9 to 15 hours of structured clinical treatment per week across three to five sessions. Day and evening scheduling allows clients to maintain employment and family responsibilities throughout the treatment course.
IOP is the evidence-supported step-down from Partial Care for clients progressing through the clinical continuum.
Outpatient Program
The outpatient program provides ongoing weekly clinical contact for clients maintaining early recovery or transitioning from IOP. It sustains clinical momentum while restoring full daily functioning without structured daily programming.
Virtual Treatment
A virtual treatment option delivers HIPAA-compliant therapy, psychiatric care, and group programming remotely for clients who cannot attend in person due to geography, employment, or caregiving responsibilities.
Step 4: What a Typical Day in Treatment Looks Like
A treatment day at Archangel Centers is structured from arrival to departure, eliminating the unstructured time that consistently elevates early relapse risk in individuals with active substance use disorder.
Morning Programming
Morning sessions typically include:
- Large group programming covering psychoeducation, recovery skill development, and CBT-based cognitive restructuring with clinician facilitation across the full group.
- Mindfulness-based awareness practice integrated into the morning structure as a regulated nervous system intervention, not as a standalone wellness add-on.
- Caseload or small group sessions of six to eight clients at the same treatment stage, facilitated by the primary therapist who follows that group throughout the program.
Afternoon Programming
Afternoon sessions typically include:
- Individual therapy sessions conducted biweekly on rotating schedules, covering personal treatment plan goals, trauma-informed intervention where clinically indicated, and progress review.
- Dialectical behavior therapy skills training covering distress tolerance, emotional regulation, interpersonal effectiveness, and mindfulness practice as formal DBT modules.
- Specialized programming addressing relapse prevention planning, trigger identification, boundary setting, and the practical skill development required for independent recovery after discharge.
Step 5: Mental Health Treatment and Dual Diagnosis Care
Mental health treatment is integrated throughout every level of care at Archangel Centers — not offered as a separate track for those who qualify.
How Dual Diagnosis Treatment Works
Integrated dual diagnosis treatment addresses substance use disorder and co-occurring psychiatric conditions within the same clinical framework and the same treatment day, rather than routing each condition to a separate program sequentially.
A psychiatrist or psychiatric nurse practitioner conducts regular medication reviews throughout the program. Medication management for co-occurring conditions including major depressive disorder, generalized anxiety disorder, bipolar disorder, and PTSD continues without interruption during active substance use disorder treatment.
Evidence-based modalities delivered across both individual and group therapy formats include cognitive behavioral therapy, dialectical behavior therapy, and trauma-informed interventions where clinically indicated. EMDR is available through a trained clinician for clients with documented PTSD presentations.
Step 6: Aftercare and Discharge Planning
Discharge planning begins on day one of treatment, not in the final week, because the period immediately after leaving structured programming carries the highest relapse risk in the full treatment continuum.
What an Aftercare Plan Covers
A structured aftercare plan addresses all of the following:
- Step-down programming: coordination of the next appropriate level of care, whether IOP, outpatient, or virtual treatment, before the current program ends.
- Psychiatric continuity: confirmed referrals for ongoing medication management or individual therapy after discharge.
- Recovery environment: sober housing recommendations where indicated, peer support group connection, and identification of local recovery resources.
- Relapse prevention: a written individualized relapse prevention plan covering specific triggers, early warning signs, and a documented response protocol.
Treatment at Archangel Centers in New Jersey
Archangel Centers provides Partial Care, IOP, outpatient, and virtual treatment for substance use disorder and co-occurring mental health conditions in Tinton Falls and East Windsor, New Jersey. Same-day assessments are available for qualifying adults.

Accepted insurance includes Aetna, Blue Cross Blue Shield, Cigna, Humana, and TRICARE. Clients can verify their insurance coverage before confirming a start date for the admissions process.
Frequently Asked Questions
What happens on the first day of rehab?
The first day begins with a clinical intake assessment covering substance use history, mental health history, medical history, and social context. Standardized screening tools including the PHQ-9 and GAD-7 quantify psychiatric symptoms. ASAM Level of Care criteria then determine which program is the appropriate starting point. (47 words)
What is the difference between PHP and IOP?
PHP, or Partial Hospitalization, provides 20 to 30 structured clinical hours per week and is classified at ASAM Level 2.5. IOP provides 9 to 15 hours per week at ASAM Level 2.1. PHP is the higher intensity level, typically completed before transitioning into IOP. (45 words)
Do you have to go to detox before rehab?
Not always. Medical detox is required only for clients physically dependent on alcohol, benzodiazepines, or opioids where cessation without pharmacological management carries serious medical risk. Stimulant and cannabis use disorders do not produce physiological withdrawal requiring detox before outpatient treatment begins. (43 words)
What does a typical day in rehab look like?
A typical treatment day includes large group psychoeducation, caseload or small group therapy with a primary therapist, individual therapy on a rotating biweekly schedule, DBT skills training, relapse prevention programming, and mindfulness-based awareness practice. The full day runs from morning through mid-afternoon with structured programming throughout. (47 words)
What is dual diagnosis treatment?
Dual diagnosis treatment addresses substance use disorder and a co-occurring psychiatric condition such as major depressive disorder, PTSD, or bipolar disorder simultaneously within the same clinical framework. Integrated treatment produces better outcomes than treating each condition sequentially in separate programs. (42 words)
How long does addiction treatment take?
Treatment length is clinically driven and varies by individual presentation. Partial Care typically runs 30 to 45 days. IOP follows for an additional 30 to 60 days. Total structured treatment engagement of 60 to 90 days produces significantly better long-term outcomes than shorter episodes per NIDA guidelines. (48 words)
Does insurance cover addiction treatment?
Most major private insurance plans cover addiction treatment at varying levels depending on the policy and deductible. Aetna, Blue Cross Blue Shield, Cigna, Humana, and TRICARE are accepted at Archangel Centers. Verifying benefits before starting confirms exactly what is covered under a specific plan. (45 words)
References
- National Institute on Drug Abuse. (2023). Principles of Drug Addiction Treatment: A Research-Based Guide (Third Edition). National Institutes of Health. https://nida.nih.gov/publications/principles-drug-addiction-treatment-research-based-guide-third-edition
- Substance Abuse and Mental Health Services Administration. (2023). Key Substance Use and Mental Health Indicators in the United States. U.S. Department of Health and Human Services. https://www.samhsa.gov/data/
- American Society of Addiction Medicine. (2023). The ASAM Clinical Practice Guideline on the Management of Opioid Use Disorder. American Society of Addiction Medicine.
- National Institute on Drug Abuse. (2020). Drug Misuse and Addiction. National Institutes of Health. https://nida.nih.gov/publications/drugs-brains-behavior-science-addiction/drug-misuse-addiction
- Centers for Disease Control and Prevention. (2023). Alcohol and Public Health: Excessive Alcohol Use. U.S. Department of Health and Human Services. https://www.cdc.gov/alcohol/
- McLellan, A. T., et al. (2000). Drug dependence, a chronic medical illness. JAMA, 284(13), 1689–1695
